

…Sir Winston Churchill’s analysis of the American way of addressing challenges. Was he correct? And if so, do his observations reflect our current approach to healthcare reform? How many alternatives to the delivery of healthcare are we bound to test before we get it right? Getting it right is of utmost importance to all of us—life and death decisions could be in the balance.
There are basically two reasons why we are embarking upon this overhaul:
The first reason is the humanitarian need to provide healthcare for those who cannot afford it. Some have asked, “Where in the Constitution does it say that the country is obligated to provide healthcare for everyone?” The answer is that it probably does not. But, just because the Constitution doesn’t provide for an action or service, does that mean that it should not be provided? You may have heard about the elementary-school-aged boy from an economically depressed background who was bounced from one hospital emergency room to another until he died of overwhelming sepsis. The boy had an abscessed tooth…but no insurance. True story! Certainly, civilization in the United States has progressed to the point that instances like this should not occur, and it is society’s responsibility to see that they don’t.
The other basic reason to overhaul the system is the impact healthcare is having on the standing of the United States on the world economic stage. The U.S. dollar is losing its credibility and value internationally as the world’s reserve currency for international business. OPEC countries, as well as India, China, Russia, the European Union and others, are taking steps to move to another currency, basket of currencies, or virtual currency for international trade, leaving the dollar behind. Dependence upon the dollar worldwide has contributed to the demand for it and support of its value. If the rest of the world loses faith in the greenback and moves to another reserve currency, the value of the dollar will fall. Some might consider that a good thing, but it could mean falling into a bottomless pit, especially when other economies are coming out of the recession faster than we are. Also, what if other countries decide there are safer havens around the world than U.S. government financial obligations and pull out the $3.5 trillion in Treasury securities they now hold? Foreign investors also own real estate and other securities in this country. What if they decided that the investment is too risky and unload those assets?
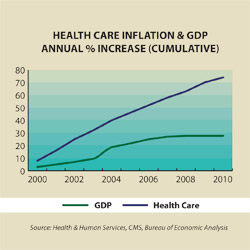
President Obama has said that we must get healthcare costs under control before we can address the financial crisis. Healthcare accounts for approximately 17 percent of the Gross Domestic Product (GDP) and is growing at around seven percent per year, while the GDP is only growing at two percent or less per year. Healthcare also accounts for approximately 15 to 20 percent of government expenditures.
While we agree with President Obama that healthcare costs must be controlled in order to address our other economic problems, we do not believe that the economic case has been clearly and comprehensively laid out to the American public. Maybe, the administration is afraid that, as Jack Nicholson said in A Few Good Men, “You [we] can’t handle the truth!”
 Healthcare costs in the United States average twice as much per capita as the average in the European Union countries. There is no doubt that the U.S. system of healthcare is riddled with the costs of waste, fraud and abuse. We should be attacking these problems seriously and putting the money in the bank for future needs. For, if we ignore the gold in the system waiting to be mined, we are bound to resort to healthcare rationing—based upon age and not evidence-based medicine.
Healthcare costs in the United States average twice as much per capita as the average in the European Union countries. There is no doubt that the U.S. system of healthcare is riddled with the costs of waste, fraud and abuse. We should be attacking these problems seriously and putting the money in the bank for future needs. For, if we ignore the gold in the system waiting to be mined, we are bound to resort to healthcare rationing—based upon age and not evidence-based medicine.
At this point, it is important to point out that those who want to change the system challenge the quality of healthcare in the United States. They point out international comparisons of infant mortality, longevity, cancer survival, mortality between the ages of one and five, and the United States’ being listed as 37th by the World Health Organization. The truth is that the unfavorable rankings are due to the way the data is counted and recorded, societal and cultural issues, the cherry-picking of data, and self-serving study designs. Space does not allow a full explanation here; however, all of these issues, and others, are discussed in our book, Reasoned Health Care Reform. It is available on amazon.com, at I Know You Like a Book in Peoria Heights, and on our website, cranegilmore.com. When people in other parts of the world, including the European Union, are faced with serious health conditions, they come to the United States for care—if they can afford it.
We spent one-and-a-half years looking into original documents from which the poor-quality assertions were made, and concluded that the data is misquoted to support somebody’s agenda. This led us to an exploration of where the dollars for healthcare are spent, who spends them, who receives them, what the administrative costs are, who is getting rich, and whose ox is getting gored. As we pursued and digested volumes of data, it became apparent that there is more than enough money in the system to pay for all of the uninsured and underinsured and still have hundreds of billions of dollars left over each year. If we could recoup those wasted dollars, we would be taking a giant step toward financial stability for the nation. Unfortunately, as our elected representatives have tried to develop a solution, special interests have taken control and we have lost sight of our two goals. Are we proving Sir Winston right again?
As we have followed the various healthcare bills introduced in Congress, we were pleased to find that many of them contained recommendations made in our book. As the 10 or so various bills and their markups have been reduced to two, we find that many of the true cost-cutting provisions that would not affect quality have been removed to try to satisfy all the major players. Here are a few examples:
 Malpractice/Defensive Medicine. The Republican House Bill HR3400 provided for protections against liability if the practice was within established guidelines. It provided expert panels and administrative healthcare tribunals to determine if cases were within the guidelines. It called for caps on noneconomic damages of $250,000. Reasoned Health Care Reform recommends specialty society-developed protocols. Panels of specialists with expertise in the area of medicine in question would determine if the protocols were being followed. If the protocols were followed, the case would go no further. Any cases outside of protocols that do go further would follow the doctrine that the “loser pays all costs.”
Malpractice/Defensive Medicine. The Republican House Bill HR3400 provided for protections against liability if the practice was within established guidelines. It provided expert panels and administrative healthcare tribunals to determine if cases were within the guidelines. It called for caps on noneconomic damages of $250,000. Reasoned Health Care Reform recommends specialty society-developed protocols. Panels of specialists with expertise in the area of medicine in question would determine if the protocols were being followed. If the protocols were followed, the case would go no further. Any cases outside of protocols that do go further would follow the doctrine that the “loser pays all costs.”
We are of the opinion that caps on noneconomic damages will not significantly affect healthcare costs. It is the defensive medicine with needless specialist referrals, extra tests, biopsies and other procedures, which have risks in and of themselves, that help drive healthcare costs. Physicians fear malpractice suits because of the publicity and time for both themselves and their office staff to prepare a defense. The mere lowering of malpractice premiums will not significantly affect the nine percent of healthcare costs due to the defensive practice of medicine (U.S. Government Office of Technology Assessment). Surveys of physicians in surgical specialties indicate that 40 to 60 percent of the increase in healthcare costs are due to defensive medicine. If we assume that only 10 percent of healthcare costs are due to the practice of defensive medicine, and through major tort reform as mentioned above, we can positively affect 70 percent, the savings would be over $175 billion per year. Why has Congress taken tort reform off the table?
- End of Life. The Democrat House Bill HR3200 provided for physician reimbursement for counseling every five years to discuss advance directives. It would also provide for more frequent reimbursement if the patient’s condition warranted. Somehow, this provision got twisted into “death panels” deciding who would live and who would die. Because of all the negative publicity and screaming at town hall meetings, the issue has been dropped. This is indeed a shame when so many healthcare dollars (27 percent of the Medicare budget) are spent in the last year of life. Many times there are no advance directives and the family cannot make any decision other than, “Doctor, do all that you can,” especially if Medicare is going to pay for it. Often, physicians are frustrated to see healthcare dollars wasted on hopeless causes, but their hands are tied. We believe that a more reasoned approach to end-of-life issues would result in annual savings of at least $45 billion.
- Risky Behavior. The Senate Finance Committee bill called for a 50-percent increase in premium for smokers. It also called for programs to help smokers quit. The increase in premium has been removed from all subsequent iterations. It is our opinion that the individual should be responsible for costs incurred by the voluntary assumption of risky behavior through increased premiums for healthcare. This is already the case for life insurance, why not for health insurance? Also, HIPAA non-discriminatory regulations already allow for an increase in healthcare premiums for risky behaviors under their standards-based provisions. Should society be saddled with the medical costs resulting from smoking, sky diving, racecar driving or motorcycle riding? We think not! Society needs to encourage responsibility for one’s self, and the individual must learn to “pay for his or her own thrills.”
- Revenue from Providers. Someone please help us understand how adding a tax to providers is going to lower healthcare costs. The Senate bill HR3590 amended version calls for annual fees or excise taxes based on sales of drug manufacturers, device manufacturers and insurance companies. Won’t these taxes ultimately be included in the cost of healthcare? Now get this—the Congressional Budget Office includes it as revenue to offset the cost of healthcare reform. When these special-interest groups were fighting for a place at the table several months ago, is this what they had in mind when pledging “their contribution” to healthcare reform?
Does Healthcare Fit the Free Market Model?
While giving a presentation on Reasoned Health Care Reform to a group of primary care physicians, we asked if anyone could remember having had a patient question the price of services or negotiate fees. The answer: NONE! In a free market, almost everyone is price-conscious. They make informed decisions after due consideration whether or not to purchase goods or services. A variety of suppliers are always willing to offer discounts to obtain the business. Monopolies are illegal except, of course, utilities. By the way, Congress is now considering treating banks as utilities in order to exert tighter control. Does healthcare fit the free market model, or is it unique? Consider these observations.
- Insurance. The beneficiary of medical care is rarely the one who actually pays for the services. Frequently, the beneficiary is not even the one who pays the lion’s share of the premium. What if insurance companies were treated as national utilities with the ability to sell their product across state lines, eliminating the administrative cost of individual state mandates? (Currently there are over 1,800 individual state mandates.) The current administrative cost for insurance companies runs between 17 and 24 percent. Of course, those administrative costs include some golden parachutes and exit packages in excess of $100 million for top executives. If the insurance companies were highly regulated on a national basis, and all offered the same basic policy, costs would go down. In Reasoned Health Care Reform, we estimate achievable savings of $128 billion per year.
- Pharmaceuticals. Is the pharmaceutical industry market- or need-driven? Many decisions at the upper levels are based on the market for a drug rather than the need. After all, the pharmaceutical companies are for-profit, meaning they exist for the benefit of the stockholders, and the executives are employed by the stockholders. A perfect example is statins to lower cholesterol. It is a huge market and growing rapidly with 17 brands including various combinations with other drugs. All do approximately the same thing.
Another example is the huge market for proton pump inhibitors that reduce acid reflux. Remember that Nexium, the little purple pill, hit the market when Prilosec’s patent ran out. Essentially the same two drugs. Wouldn’t it be great if the Institutes of Medicine or some other responsible governmental agency, immune from the politics, determined the drugs needed and funded contracts for research and development. Once the drug is developed, the people of the United States own the patent and determine the cost of the drug based upon a reasonable profit for the manufacturer through a bidding process. The U.S. would derive a percentage of the profit from overseas sales. The same scenario could apply to the manufacture of medical devices. Remember, we currently own a part of General Motors and several financial institutions. Why not?
- Hospitals. Currently, hospitals spend 13 percent of their income on collecting what is due. If everyone were covered by at least a basic, comprehensive policy nationwide, the need to argue and negotiate with insurance company claims adjusters would be greatly reduced. The same is true for physician offices. Physicians and their staff spend an inordinate amount of time obtaining coverage for procedures and tests. We estimate a realistic savings of at least $51 billion per year in hospital administrative costs alone.
- Physician/Patient Relationship. When the anesthesiologist visits the patient awaiting outpatient surgery, is that the time to discuss fees, challenge credentials or shop for a better deal? The relationship between any physician and his or her patient is an extremely private and personal relationship. Not the type of relationship established between a free market buyer and seller.
- Competition. A little competition is always a good thing. In the realm of healthcare, too much competition drives healthcare costs up. For example, one hospital adds a new sub-specialty wing. In response, another makes all rooms private, while another in the area buys a helicopter, and the costs keep spiraling upward. Pharmaceuticals increase demand through direct-to-consumer advertising and all-expense-paid outings at golf resorts. Is society better off when parents and their children are watching a prime time family television show when the commercial break promotes a treatment for erectile dysfunction? “Mommy, what’s…?”
A unique business model is needed at this time in the evolution of healthcare. Decisions should be based upon the actual needs of society, and not so much on profit motive, market share and competition.
How Has the Healthcare Free Market Model Influenced the Process?
Because healthcare is big business, the stakeholders have been very active—wheeling and dealing, making backroom deals, and lobbying for self-interests. Here are only a few examples:
- The public option has been out, in, out, and back in, depending upon the day. It is true that the playing field is not level when comparing a government-subsidized public option with private insurance. Why couldn’t there be a level playing field and include a public option to provide a little cost and quality competition? Admittedly, many things would need to be changed, including accounting for private insurance taxes and reserves, versus none for government-run programs.
- In exchange for support of the Senate bill, the American Medical Association negotiated a substitution of the five-percent tax on elective cosmetic surgery for a 10-percent tax on tanning parlors to help pay for healthcare reform. Was there an agreement that the AMA would retain exclusive rights to healthcare coding bringing in tens of millions of dollars per year?
- A few physician-owned hospitals, currently under construction, will be exempted from some transparency provisions related to grandfathering, based upon date of completion.
- Pharmaceutical companies support reform, but a rumored trade-off is that the current Medicare drug pricing formulas will not be used in the new public option (if there is one) and a ban on importation of cheaper foreign drugs.
- Insurance companies agreed to no denial of coverage for pre-existing conditions in exchange for mandatory health insurance. This would generate an additional estimated $240 billion per year for the insurance companies.
- Trial lawyers, generous political contributors, objected to significant tort reform…none being contemplated.
Get the idea?
Everyone agrees we need healthcare reform. Each organization and each individual is all for it, as long as they are not adversely affected. If we made our decisions based upon the needs of the country as a whole, rather than the wants and desires of the interested parties, we could cover everyone, put money in the bank, and help to improve the status of the dollar internationally. iBi
Crane Gilmore & Associates, Inc. are consultants in healthcare cost containment, health promotion, benefit plan design and workers’ compensation. Visit cranegilmore.com for more information.
